The Hidden Figure in the Drug Price Epidemic: Pharmacy Benefit Managers
Written by SNAP member Mikayla Smith-Craven
Footnotes are denoted with superscript. References are denoted with brackets.
“Do you take GoodRx?”
This was a question I received regularly while working as a pharmacy intern in Bonner Springs, Kansas. Patients would come up to the counter to pick up their medications, hear the cost, and immediately pull up the discount prescription website to search for a coupon that matched the prescription written by their doctor. While this situation was almost guaranteed to occur for uninsured patients, many insured patients also utilized the tool. They often found that their co-pays, or out-of-pocket costs, were significantly greater than the price promised by GoodRx. In 2024, GoodRx reported that 30 million Americans saved by using their service: approximately 10% of the U.S population [1].
Over the course of my three and a half years at that pharmacy, I helped countless patients find their way through the maze of health insurance and other alternatives like GoodRx, but the root cause of the high prescription cost crisis in America is not so easily discovered as a prescription coupon.
There are many factors that go into setting the out-of-pocket costs patients pay for their prescription medications, including pharmaceutical companies, drug manufacturers, insurance companies, and pharmacies; yet, one crucial piece of the puzzle often escapes scrutiny by the public: the middleman of the pharmaceutical industry.
A middleman in many industries is the point of control between two other entities. In most circumstances, the middleman has a lot of power. They control the process of getting a product or service from one entity (often a business) to another (often a consumer). Middlemen stay largely anonymous, or at least unreachable, by the consumer, yet they often receive compensation from both parties. This allows them to achieve significant profit.
Pharmacy benefit managers (PBMs) are the middlemen of the pharmaceutical industry and are one of the primary forces keeping drug prices so high for consumers, even those with insurance. Have you ever gone to the pharmacy, prescription in hand, only to hear that your medication requires prior authorization, and were bewildered to discover that your insurance company refused to cover the medication unless they received further description of need for the medication by your doctor?¹ This situation, where the power to decide which medication is right for you, lies with the PBMs, rather than with you or your trusted physician, is one symptom of the rebate system for drug costs employed by PBMs.
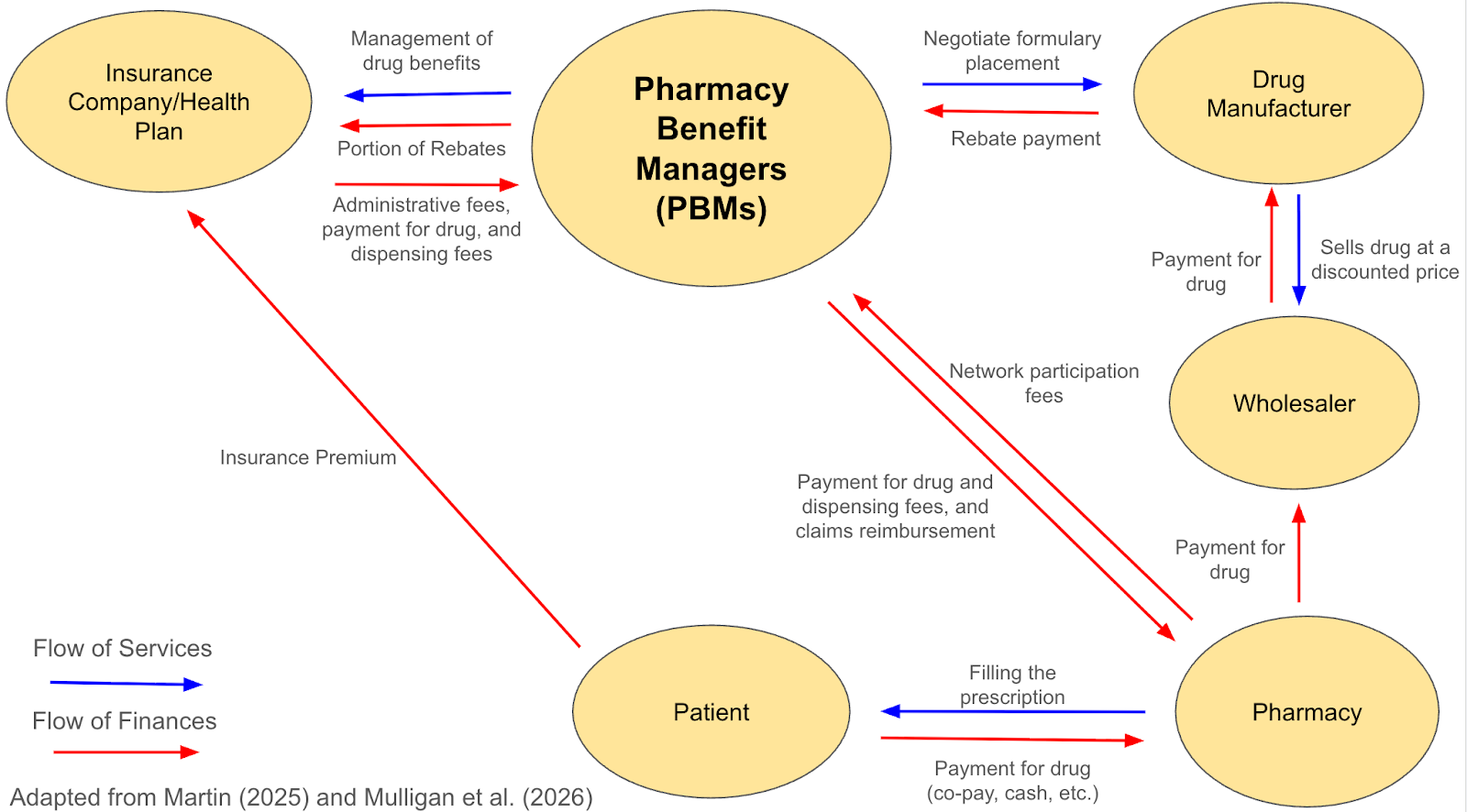
Figure 1: An overview of the flow of finances and services between the various stakeholders of the drug pricing structure. PBMs are the point of control between the insurance company/health plan, drug manufacturer, and pharmacy. [2, 3]
Through this rebate system, PBMs negotiate discounts and rebates with drug manufacturers in exchange for favorable placement of certain drugs on insurance formularies, which are the lists of drugs covered by a health plan. While these rebates were intended to lower costs when they were introduced in the 1980s and 1990s, over time, they have evolved [4]. Today, they serve as an insignificant hurdle at best, with drug manufacturers simply setting the prices of drugs artificially high to offset expected rebates, and an anti-consumer limiting tool at worst, with these rebates often dictating which pharmacy you can go to and what medications qualify for insurance coverage [4]. PBMs then make a profit off of “the spread”, which is the difference between the administrative fees and payment for drug and drug dispensing paid to PBMs from the insurance company or health plan, and the reimbursement the PBMs pay to pharmacies who dispense the medication (Figure 1).
It is clear that PBMs no longer negotiate these discounts for the benefit of patients. Instead, they are focused on ensuring maximum profit for themselves, insurance companies, drug manufacturers, and large-scale pharmacies that they were initially intended to police. How did this happen? Acquisitions resulting in healthcare conglomerates that have stakeholders at each level of the process have driven this change. The resulting system means the price patients see at the pharmacy counter bears little resemblance to the drug’s actual production cost, benefiting those who manage the process rather than those in need of the medication [5].
Unfortunately, many proposed policy solutions don’t adequately address the structural issues underlying these high prices. The focus often lies on reducing the sticker price of the medication by targeting pharmaceutical companies and drug manufacturers, as was the case for the Inflation Reduction Act of 2022 and the more recent Most-Favored-Nation Executive Order from 2025 [6-8]. However, this narrow focus fails to account for the power of the PBMs and other aspects of the system that impact the out-of-pocket price paid by patients. The power to decide whether a medication will even be on the formulary and if so, which insurance tier, whether insurance will cover it at your local pharmacy, and whether it will require a prior authorization (despite a licensed physician prescribing it to you) lies with the PBMs. To address the complex system driving high prices for patients, reform will require a nuanced approach that considers all parties involved, especially those that have previously evaded public scrutiny, such as the US patent system and PBMs.²
We need greater transparency for drug pricing. Specifically, laws that require PBMs and pharmaceutical companies to disclose pricing structures, rebate amounts, and profit margins would help patients and policymakers understand the true drivers of drug costs [9]. A newly proposed rule by the US Department of Labor on January 29, 2026 would require PBMs to disclose compensation they receive from drug manufacturers and pharmacies, and how that compares to the rebates or discounts that they are providing to pharmacies. This rule would also allow for financial representatives of insurance plans to audit the accuracy of these disclosures made by PBMs [10]. This rule indicates a growing political awareness towards the role of PBMs as the bottleneck of the drug pricing system, which hopefully will allow for a more comprehensive review of the overall healthcare system in the US.
So many patients, both insured and uninsured, are rightfully frustrated and angry about the state of prescription drug pricing in the United States. Patients should not have to rely on prescription coupon websites, such as GoodRx, to afford their medications. By examining PBMs and the unnecessary power they wield over the American healthcare system, we can start to build a system that prioritizes patient well-being over profits and ensures that essential medications are affordable for all.
Overall, the issue of high prescription drug prices stems from a system designed to be opaque and complex for patients, as well as favorable to intermediaries, like PBMs. Addressing this crisis requires a comprehensive approach that considers every layer of the pricing process, even the elusive middlemen.
Recognition:
Mikayla Smith-Craven holds a doctorate in Pharmaceutical Chemistry from the University of Kansas where she focused on drug development and delivery of life-saving medications amphotericin B and zidovudine.
Special thanks to fellow SNAP members who provided feedback on this blog: Emily Selland, an ecologist and public health scientist whose research focuses on sustainable and economically viable innovations for infectious disease control; Edith-Marie Green, a population health scientist whose research focuses on aging and end-of-life healthcare, as well as global health and the rural-urban continuum; and Shaurita D. Hutchins, a PhD candidate in Genetics, Genomics, and Bioinformatics focused on advancing rare disease diagnostics and ethical genomics data stewardship.
Footnotes:
- The American Medical Association survey results reported that in 2024, practices saw an average of 39 prior authorizations per physician per week and an average of 13 hours completing those requests per week [11].
- For more information on how the US patent system and the concept of “evergreening” impact out-of-pocket costs for patients, please read the following articles: Gurgula O. (2020); Feldman (2018); UC San Francisco Law (2020)
References:
- GoodRx (2024). The GoodRx Effect. Accessed March 2026.
- Martin, K. (2025). What Pharmacy Benefit Managers Do, and How They Contribute to Drug Spending. Commonwealth Fund.
- Mulligan, K.; Lakdawalla, D. (2026) Hidden Profits? How Accounting Conventions and Vertical Consolidation Can Obscure PBM Profitability. University of Southern California Leonard D. Schaeffer Institute for Public Policy and Government Service.
- Gale A. (2023). If Pharmacy Benefit Managers Raise Drug Prices, Then Why Are They Needed? Missouri Medicine, 120(4), 243–244.
- U.S. Federal Trade Commission Office of Policy Planning (2024). Pharmacy Benefit Managers: The Powerful Middlemen Inflating Drug Costs and Squeezing Main Street Pharmacies. Interim Staff Report.
- The 117th US Congress (2021-2022). H.R.5376 - An act to provide for reconciliation pursuant to title II of S. Con. Res. 14.
- U.S. Government Accountability Office (2025). Inflation Reduction Act of 2022: Initial Implementation of Medicare Drug Pricing Provisions. GAO-25-106996.
- The White House (2025). Delivering Most-Favored-Nation Prescription Drug Pricing to American Patients.
- Seeley, E.; Kesselheim, A. (2019). Pharmacy Benefit Managers: Practices, Controversies, and What Lies Ahead. Commonwealth Fund.
- Employee Benefits Security Administration (2026). US Department of Labor proposes historic pharmacy benefit manager fee disclosure rule. US Department of Labor.
- Albert Henry, T. (2025) Fixing prior auth: Nearly 40 prior authorizations a week is way too many. American Medical Association.